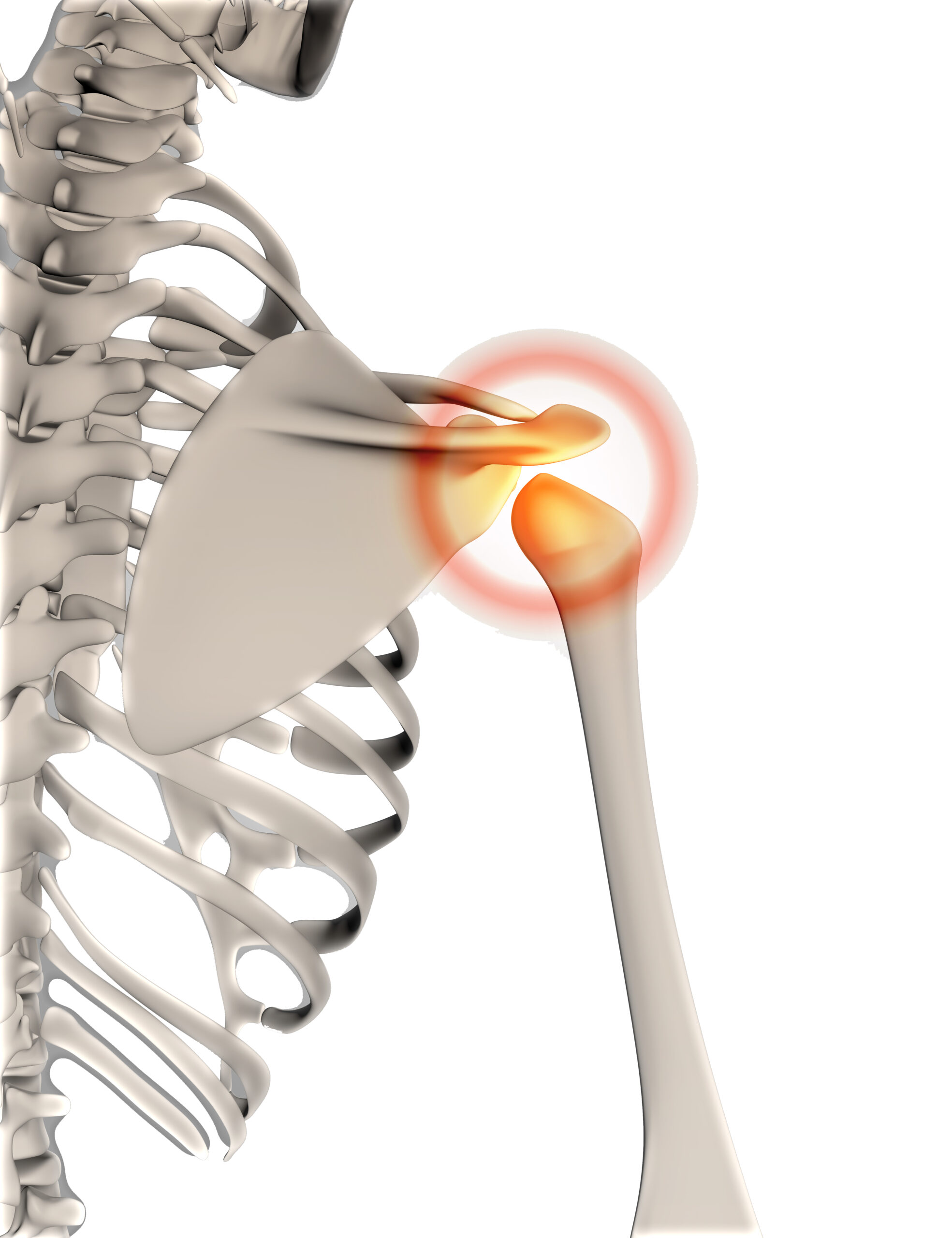
Frozen Shoulder
Frozen shoulder, also called adhesive capsulitis, causes pain and stiffness in the shoulder. Over time, the shoulder becomes very hard to move.
After a period of worsening symptoms, frozen shoulder tends to get better, although full recovery may take up to 3 years. Physical therapy, with a focus on shoulder flexibility, is the primary treatment recommendation for frozen shoulder.
Frozen shoulder most commonly affects people between the ages of 40 and 60, and occurs in women more often than men. In addition, people with diabetes are at an increased risk for developing frozen shoulder.